The Bristol GDNF results


|
Today – 27th February, 2019 – the long-awaited results of the Phase II GDNF clinical trial were published. GDNF (or glial cell line-derived neurotrophic factor) is a protein that our bodies naturally produce to nurture and support cells. Extensive preclinical research suggested that this protein was particularly supportive of dopamine neurons – a group of cells in the brain that are affected by Parkinson’s. The results of the Phase II clinical trial suggest that the treatment was having an effect in the brain (based on imaging data), but the clinic-based methods of assessment indicated no significant effect between the treatment and placebo groups. In today’s post we will look at what GDNF is, review the previous research on the protein, discuss the results of the latest study, and look at what happens next. And be warned this is going to be a long post! |
 Boulder, Colorado. Source: Rps
Boulder, Colorado. Source: Rps
It all began way back in 1991.
George H. W. Bush was half way into his presidency, a rock band called Nirvana released their second album (‘Nevermind’), Michael Jordan and the Chicago Bulls rolled over the LA Lakers to win the NBA championship, and Arnold Schwarzenegger’s ‘Terminator 2’ was the top grossing movie of the year.
 Source: Stmed
Source: Stmed
But in the city of Boulder (Colorado), a discovery was being made that would change Parkinson’s research forever.
In 1991, Dr Leu-Fen Lin and Dr Frank Collins – both research scientists at a small biotech company called Synergen, isolated a protein that they called glial cell-derived neurotrophic factor, or GDNF.
And in 1993, they shared their discovery with the world in this publication:
 Title: GDNF: a glial cell line-derived neurotrophic factor for midbrain dopaminergic neurons.
Title: GDNF: a glial cell line-derived neurotrophic factor for midbrain dopaminergic neurons.
Authors: Lin LF, Doherty DH, Lile JD, Bektesh S, Collins F.
Journal: Science, 1993 May 21;260(5111):1130-2.
PMID: 8493557
For the uninitiated among you, when future historians write the full history of Parkinson’s, there will be no greater saga than GDNF.
In fact, in the full history of medicine, there are few experimental treatments that people get more excited, divided, impassioned and evangelical than GDNF.
This ‘wonder drug’ has been on a rollercoaster ride of a journey.
What exactly is GDNF?
GDNF stands for glial cell-derived neurotrophic factor.
Let’s break that down.
Glial cells are the support cells in the brain. While neurons are considered to be the ‘work horses’ of neurological function – passsing messages and storing memories – glial cells are in the background making sure that neurons are supported, protected and nurtured.
There are different types of glial cells, including astrocytes, oligodendrocytes and microglia. And each type has a specific function, for example microglia are the brain’s resident immune cells checking up on the health of the neurons while oligodendrocytes provide the neurons with a protective covering (called myelin sheath) which also helps to speed up the signalling of neurons.
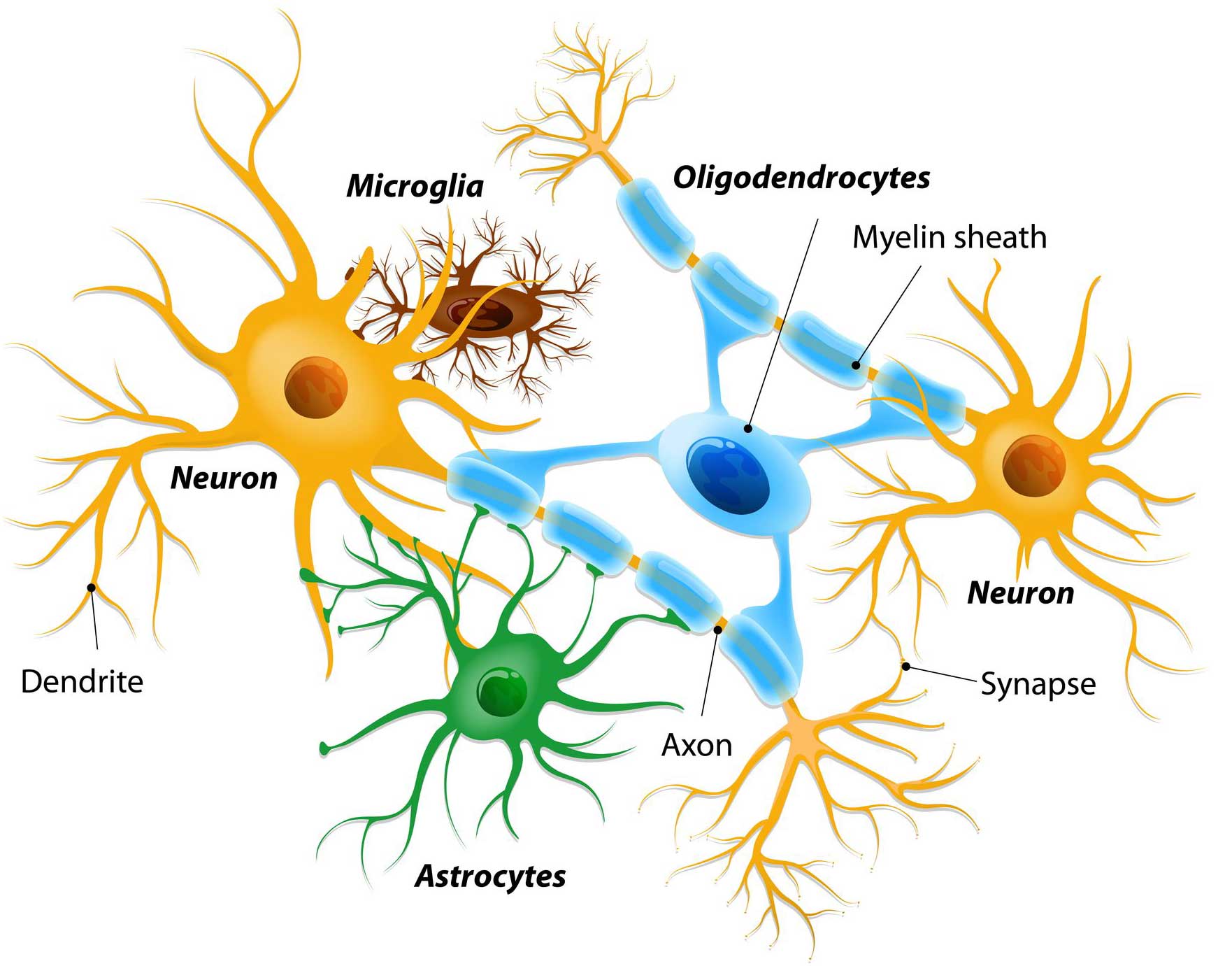 Different types of cells in the brain. Source: Dreamstime
Different types of cells in the brain. Source: Dreamstime
Astrocytes provide nutrients to neurons and make sure the environment surrounding the neurons is balanced and supportive. Glial cells are absolutely critical to the normal functioning of the brain.
So that is the “glial cell” part of glial cell-derived neurotrophic factor, now let’s focus on the latter part.
Neurotrophic factors (neurotrophic = Greek: neuron – nerve; trophikós – pertaining to food/to feed) are chemicals that nurture neurons and support growth. There are many types of neurotrophic factors, some having more beneficial effects on certain types of neurons and not other. GDNF is one of these neurotrophic factors.
Dr Leu-Fen Lin and Dr Frank Collins (who I mentioned above) isolated GDNF from a cell culture of rat glial cells – hence the name: glial cell-derived neurotrophic factor.
 The structure of GDNF protein. Source: Wikipedia
The structure of GDNF protein. Source: Wikipedia
GDNF is a member of a larger family of neurotrophic factors.
And there are three other members of that family (called neurturin, persephin, and artemin – sounds like the Three Musketeers!) have also demonstrated positive effects on dying dopamine neurons. The positive/neuroprotective effect of these neurotrophic factors works via a series of ‘receptors’ on the outer surface of cells. Receptors are molecules sitting on the surface of cells, waiting for specific proteins to come along and bind to them. By binding to them, the receptor becomes activated.
There are receptors that are specific for each of the GDNF family members, and when they bind to their respective receptor, they activate another surface protein called RET.
 The GDNF family photo. Source: Nature
The GDNF family photo. Source: Nature
Ret proto-oncogene (or RET) is a receptor tyrosine kinase, that is a cell-surface molecule that initiates signals inside the cell after surface receptors are bound. The activation of RET results in cell growth and survival. Dopamine neurons in our brains have most of the GDNF family receptors and a lot of RET.
GDNF has its neuroprotective effect on dopamine neurons by activating its receptor, which activates RET (Click here for a very good OPEN ACCESS review of GDNF biology).
How much research has been conducted on GDNF in Parkinson’s?
A LOT!
GDNF has to be one of the most researched compounds for potential therapeutic use in Parkinson’s, because so much of the early data that was generated was so impressive.
[And this is where the roller coaster ride starts…]
One year after the original Lin and Collins GDNF report, the first reports of the neuroprotective properties of GDNF in animal models of Parkinson’s began to be reported (Click here, here and here for the first reports), and another year after that the first report of beneficial effects in non-human primate models of Parkinson’s were published (Click here to read more about this).
And it’s important to understand that these results have been independently replicated many, many times (Click here, here and here for some early examples). There is a great deal of research investigating all aspects of GDNF in models of Parkinson’s (Click here to read a good OPEN ACESS review of this topic).
[…the rollercoaster was heading up to lofty heights…]
As a result of all this positive data, a lot of members of the Parkinson’s research community got very excited that perhaps Dr Lin and Dr Collins had stumbled upon the much sought after “miracle cure” for Parkinson’s.
In 1994, the biotech company Synergen was immediately swallowed up by the Pharmaceutical company Amgen, which subsequently owned the rights to GDNF and its use in Parkinson’s.
![]()
Sensing that they were on to a potentially blockbuster treatment for Parkinson’s, Amgen quickly started setting up clinical trials to evaluated whether the neuroprotective effects of GDNF would translate into humans. Between July 1996 and April 1999, 50 people with advanced Parkinson’s had tubes implanted in their heads which accessed the ventricular system of the brain.
The ventricular system is space surrounding (and within) your brain that is filled with cerebrospinal fluid – the nurturing liquid that your brain sits in.
 The ventricular system of the brain. Source: Mayfieldclinic
The ventricular system of the brain. Source: Mayfieldclinic
By putting the tube into the ventricular system and then injecting GDNF, the Amgen researchers were hoping that the GDNF would permeate and spread through the brain and find its way to the dopamine neurons.
Unfortunately, GDNF can not be given orally because it does not cross the blood brain barrier – a protective membrane surrounding the brain. But the results of the ventricular delivery approach suggested that this was not an ideal method of treatment:

Title: Randomized, double-blind trial of glial cell line-derived neurotrophic factor (GDNF) in PD.
Authors: Nutt JG, Burchiel KJ, Comella CL, Jankovic J, Lang AE, Laws ER Jr, Lozano AM, Penn RD, Simpson RK Jr, Stacy M, Wooten GF; ICV GDNF Study Group.
Journal: Neurology. 2003 Jan 14;60(1):69-73.
PMID: 12525720
The ventricular route of administration was flawed because the GDNF could not penetrate very deep into the brain, and as a result it had a very limited effect. Worse still because the cerebrospinal fluid provides access to the spinal cord and other regions of the central nervous system, numerous side effects were reported in the 38 study participants who received GDNF, including hyponatremia, nausea, vomiting, and paresthesias (prickly feeling in peripheral nerves).
The side effects led Amgen to halt the study prematurely – and unfortunately, it would not be the last time that Amgen would halt a GDNF trial.
[The GDNF rollercoast is crashing down from those initial giddy heights]
At this point, Amgen apparently shelved the drug. To their credit though, the company did make GDNF readily available to researchers seeking to work with it, but it would be another two years before any other humans were injected with it.
So what happened next?
During those years, Amgen was approached by multiple groups of researchers who were interested in conducting a clinical trial of GDNF in Parkinson’s, and the company finally agreed to supply the drug to a research team at the Frenchay Hospital in Bristol (UK).
 Bristol. Source: Megabus
Bristol. Source: Megabus
In this small clinical study, the GDNF was injected directly into the brain, into an area called the putamen. Dopamine neurons in the brain reside in an area called the substantia nigra, near the base of the brain, but they project their branches (or axons) to the several other areas, including the putamen, and this is where they release most of their dopamine.
 The projections of the substantia nigra dopamine neurons & location of the putamen. Source: MyBrainNotes
The projections of the substantia nigra dopamine neurons & location of the putamen. Source: MyBrainNotes
{kind=link}
Appreciating that the putamen is where many of the branches of the dopamine neurons can be found, the researchers in Bristol hoped that by delivering GDNF to that region they would encourage the dopamine neurons to grow more branches. An example of regenerative medicine. They recruited 5 individuals with advanced Parkinson’s and implanted tiny tubes into the putamen, which would allow for the GDNF to be pumped into that region.
And what did the results of this trial find?
The results of this small Phase I study were rather remarkable.
[The rollercoast is pulling out of the dip and heading up again]
And they shocked the Parkinson’s research world when they were published in 2003:
 Title: Direct brain infusion of glial cell line-derived neurotrophic factor in Parkinson disease.
Title: Direct brain infusion of glial cell line-derived neurotrophic factor in Parkinson disease.
Authors: Gill SS, Patel NK, Hotton GR, O’Sullivan K, McCarter R, Bunnage M, Brooks DJ, Svendsen CN, Heywood P.
Journal: Nat Med. 2003 May;9(5):589-95.
PMID: 12669033
In this study, the researchers treated the 5 participants with GDNF for one year. The findings of the study found that GDNF treatment resulted in:
- a 39% improvement in the OFF-medication motor ability (according to the Unified Parkinson’s Disease Rating Scale (UPDRS))
- a 61% improvement in how subjects perceived their ability to go about daily activities.
- a 64% reduction in medication-induced dyskinesias (and they were not observed off medication)
- no serious clinical side effects (none of the issues reported in the first study)
Importantly, the researchers conducted brain imaging studies on these participants and they reported a 28% increase in striatum dopamine storage after 18 months (based on Fluorodopa PET scans).
And then of course, there are the videos.
The videos?
This is a video of some of the patients involved in the first pilot study of GDNF. As you will see, the difference between the before and after footage is rather striking:
(If you have sound on, you can hear Tom Isaacs and Dr Stephen Gill talking about GDNF)
And the effect of the GDNF treatment appeared to have long lasting effects in these individuals, as a two year follow-up study suggested:
 Title: Intraputamenal infusion of glial cell line-derived neurotrophic factor in PD: a two-year outcome study.
Title: Intraputamenal infusion of glial cell line-derived neurotrophic factor in PD: a two-year outcome study.
Authors: Patel NK, Bunnage M, Plaha P, Svendsen CN, Heywood P, Gill SS.
Journal: Ann Neurol. 2005 Feb;57(2):298-302.
PMID: 15668979
In this study, the same 5 patients demonstrated a 57% and 63% improvement in their OFF-medication motor and activities of daily living subscores (Unified Parkinson’s Disease Rating Scale) after 2 years of treatment.
And the researchers also published a case study of one trial patient, suggesting that the positive effects of GDNF were still having an impact 3 years after the drug had stopped being delivered (Click here to read more about that report). There was also a postmortem analysis of one participants brain indicating the sprouting of dopamine fibres in the putamen (Click here for more on this).
This is amazing! So what happened next?
[The rollercoast is racing up to another peak… I wonder what could come next?]
There was one major issues with the Phase I GDNF clinical study: the trial was an open label.
Both the participants taking part in the study and the physicians conducting the study knew who was getting the drug. The study was not blind, which opens the door to the potential for a major placebo effect (more on this below).
An independent replication of the study was required and that came in 2007:
 Title: Unilateral intraputamenal glial cell line-derived neurotrophic factor in patients with Parkinson disease: response to 1 year of treatment and 1 year of withdrawal
Title: Unilateral intraputamenal glial cell line-derived neurotrophic factor in patients with Parkinson disease: response to 1 year of treatment and 1 year of withdrawal
Authors: Slevin JT, Gash DM, Smith CD, Gerhardt GA, Kryscio R, Chebrolu H, Walton A, Wagner R, Young AB.
Journal: J Neurosurg. 2007 Apr;106(4):614-20.
PMID: 17432712
In this Phase I study, 10 people with Parkinson’s were unilaterally implanted with a tube to deliver GDNF to the putamen. This means that only one side of the brain was being treated with GDNF. But after 12 months of treatment, the participants had improved by 42 and 38% in the OFF- and ON-medication states according to the total UPDRS score.
[Be warned, the rollercoaster is peaking here]
After 12 months of treatment, the participants were taken off the GDNF (the sponsor deliberately stopped the treatment based on other events – see below), but they were assessed for another 12 months. The benefits from the GDNF treatment were completely lost by 9 to 12 months after stopping the GDNF infusion (the UPDRS scores had returned to their baseline levels).
[Rollercoaster is discovering gravity again, and heading for another dip…]
More importantly, 7 of the 10 participants had apparently developed antibodies to GDNF.
What are antibodies?
Antibodies are Y-shaped proteins that the immune system naturally and continuously produces to identify anything in the body that is ‘not self’ (that is, not a normally occurring part of you – think of viruses, bacteria, etc).

Monoclonal antibodies. Source: Astrazeneca
Antibodies act like alert flags for the immune system.
When antibodies bind to something, they alert the immune system to investigate and potentially remove. The binding of an antibody to a protein can also prevent the protein from doing its function. Thankfully, this development did not result in an immune reaction in any of the participants, which could have resulted in the body attacking any source of GDNF – foreign or self.
This doesn’t sound like a good development though. What happened next?
[Gravity has hold of the Rollercoaster…]
In parallel to this small Phase I study, Amgen also initiated a double blind clinical trial for GDNF with 34 participants. Being double blind, both the researchers and the participants did not know who was getting GDNF or a control treatment. The procedure used a very different pump to deliver the GDNF into the brain (compared to the one used in the Bristol study), and some have suggested that this may have contributed to the outcome of this study.
What was the outcome of that study?
In June 2004, Amgen announced that its clinical trial testing the efficacy of GDNF in treating advanced Parkinson’s had shown a biological effect (based on Fluorodopa PET brain imaging), but failed to demonstrate any clinical improvement (compared to placebo treatment) after six months of use (Click here to read the press release).
[…and the rollercoaster is now in free fall…]
Later that year (in September), Amgen halted the study completely. They cited two reasons:
- Pre-clinical data from non-human primates that had been treated in the highest dosage group for six months (followed by a three-month washout period) exhibited a significant loss of neurons in an area of the brain called the cerebellum (which is involved in coordinating movement)
- They had detected antibodies in 18 of the 34 study participants (4 of whom had developed neutralising activity – Click here to read more about this).
The results of this study were published in 2006:
 Title: Randomized controlled trial of intraputamenal glial cell line-derived neurotrophic factor infusion in Parkinson disease.
Title: Randomized controlled trial of intraputamenal glial cell line-derived neurotrophic factor infusion in Parkinson disease.
Authors: Lang AE, Gill S, Patel NK, Lozano A, Nutt JG, Penn R, Brooks DJ, Hotton G, Moro E, Heywood P, Brodsky MA, Burchiel K, Kelly P, Dalvi A, Scott B, Stacy M, Turner D, Wooten VG, Elias WJ, Laws ER, Dhawan V, Stoessl AJ, Matcham J, Coffey RJ, Traub M.
Journal: Ann Neurol. 2006 Mar;59(3):459-66.
PMID: 16429411
What followed was an ugly chapter in the story of GDNF.
Amgen refused to allow their study participants to continue to use GDNF when they requested it on compassionate use grounds. Lawyers then got involved (two lawsuits in 2005), but the judges decided in favour of Amgen.
[…still falling]
As all of this was going on, other members of the GDNF neurotrophic factor family were being tested in models of Parkinson’s, particularly Neurturin. Much of this research used a different form of delivery – called gene therapy.
What is gene therapy?
Gene therapy is an experimental treatment approach that involves treating Parkinson’s with DNA rather than drugs.
The gene therapy involves inserting a piece (or multiple pieces) of DNA into a cell which will cause the cell to start to produce proteins that they usually do not. The introduction of the DNA is usually achieved using genetically modified viruses which have had all the disease causing component removed, allowing us to use the virus as an efficient delivery system. Viruses by their very nature are good at infecting cells so if we remove the disease causing components, what is left is a very efficient biological delivery system.
 Gene therapy. Source: Yourgenome
Gene therapy. Source: Yourgenome
[Could the rollercoaster be showing signs of going up again?]
A biotech company called Ceregene was at the leading edge of this approach and they initiated clinical trials of their gene therapy product called CERE-120.
![]() The Phase I study suggested that the treatment was safe and well tolerated (Click here to read more about this), so the company initiated a Phase II clinical trial (Click here to read the details of that study), and the results were published in 2012 (Click here to read those) with a longer-term follow up set of results being published in 2015:
The Phase I study suggested that the treatment was safe and well tolerated (Click here to read more about this), so the company initiated a Phase II clinical trial (Click here to read the details of that study), and the results were published in 2012 (Click here to read those) with a longer-term follow up set of results being published in 2015:
 Title: Gene delivery of neurturin to putamen and substantia nigra in Parkinson disease: A double-blind, randomized, controlled trial
Title: Gene delivery of neurturin to putamen and substantia nigra in Parkinson disease: A double-blind, randomized, controlled trial
Authors: Warren Olanow C, Bartus RT, Baumann TL, Factor S, Boulis N, Stacy M, Turner DA, Marks W, Larson P, Starr PA, Jankovic J, Simpson R, Watts R, Guthrie B, Poston K, Henderson JM, Stern M, Baltuch G, Goetz CG, Herzog C, Kordower JH, Alterman R, Lozano AM, Lang AE.
Journal: Ann Neurol. 2015 Aug;78(2):248-57.
PMID: 26061140
In this study, between December 2006 and November 2008, 58 patients at 9 research sites across the USA were recruited to the trial. The participants were randomly assigned to either receive bi-lateral injections in the brain of an AAV-virus containing the DNA of neurturin, or a shame surgery. But after a 15- to 24-month study, the investigators found no difference between the participants.
All of these developments (and more) left many in the Parkinson’s research community thinking that neurotrophic factors were not going to work for this condition.
[The brakes have been applied and the rollercoaster has come to a complete stop at the bottom of the dip]
And perhaps, the situation would have remained like this, if not for the dogged efforts of certain inidividuals who brought about the Phase II Bristol GDNF clinical trial.
Who were these ‘dogged’ individuals?
One of them was Tom Isaacs.
In 1996 – at just 27-years of age – Tom, a London-based surveyor, was diagnosed with Parkinson’s. After dealing with the initial shock of it all, Tom embraced his situation and became a committed, (utterly) tireless activist. He firstly walked the entire coastline of the UK to raise money and awareness for Parkinson’s.

His book, “Shake well before use“, discusses that trip and adapting to life with Parkinson’s (it is a fantastic read). Half way through his epic walk, however, the Phase I GDNF clinical trial results were published and caused a sensation. Tom was told by a friend: “You can stop walking, they have cured it”
Tom completed his walk though and upon returning to London, he (along with three others) founded and set up the Cure Parkinson’s Trust. He was a passionate advocate for GDNF and one of the driving forces behind the Phase II Bristol GDNF trial.
Another enthusiastic proponent of the GDNF approach was Prof Stephen Gill, who was the lead investigator on the Phase I clinical study which provided the original GDNF results. Prof Gill was also the inventor of the innovative delivery system used in the clinical trials.
 Prof Steven Gill. Source: Spire
Prof Steven Gill. Source: Spire
Amusing anecdote – the first time Tom Isaacs met Prof Gill was during his 2002 coastal walk as Tom was passing by Bristol. After crossing the Severn bridge, they met at the Severn View service station, bought a cup of coffee, sat down and talked about GDNF.
 The Severn View service station. Source: Geograph
The Severn View service station. Source: Geograph
A third character that deserves mention in the story of the Bristol GDNF Phase II clinical trial is Bryn Williams, founder of Funding Neuro – a charity focused on funding research that will accelerate the cures for neurological conditions. Bryn has been a passionate advocate for the Bristol GDNF clinical trial.
 Bryn Williams. Source: Herald
Bryn Williams. Source: Herald
So what was the Bristol GDNF trial?
In January 2010, while the gene therapy clinical trials were being conducted for neurotrophic factors, Amgen licenced the rights to GDNF to a company called Medgenesis.
 And the folks at Medgenesis were very keen to see another clinical trial in Parkinson’s
And the folks at Medgenesis were very keen to see another clinical trial in Parkinson’s
Together with the Cure Parkinson’s Trust & Bryn Williams, Prof Gill approached Parkinson’s UK and proposed conducting another Phase II double blind clinical study of GDNF in individuals with advanced Parkinson’s.

Parkinson’s UK agreed that it was a good idea and also agreed to fund the bulk of the study.
The new study began in 2012, and it involved a revolutionary new method of delivering the treatment, which involved tubes being implanted in the brain with pin point precision thanks to the assistance of robotics (a system developed by Prof Gill and a company called Renishaw). These tubes connected with another tube which ran to a small port which was placed just behind the ear.
 Source: Medium (a very good article from Parkinson’s UK discussing the study)
Source: Medium (a very good article from Parkinson’s UK discussing the study)
And it was via this port that the GDNF (or placebo) treatment was delivered to the participants in the study.
 A participant receiving treatment. Source: Parkinson’s UK
A participant receiving treatment. Source: Parkinson’s UK
I am often referring to “added value” being an important part of any future clinical trials, and this delivery system is a fantastic example of this. This same technology is now being used in the ongoing CDNF clinical trial for Parkinson’s being conducted in Finland/Sweden (more on this below) as well as multiple oncology clinical trials. Regards of the results of the GDNF trial, the output of the study has already had tremendous benefits (‘added value’) for the wider medical community.
Sounds very interesting. So the results of the study were published today?
Yes, in the prestigious journal ‘Brain’:
 Title: Randomized trial of intermittent intraputamenal glial cell line-derived neurotrophic factor in Parkinson’s disease
Title: Randomized trial of intermittent intraputamenal glial cell line-derived neurotrophic factor in Parkinson’s disease
Authors: Whone A, Luz M, Boca M, Woolley M, Mooney L, Dharia S, Broadfoot J, Cronin D, Schroers C, Barua NU, Longpre L, Barclay CL, Boiko C, Johnson GA, Fibiger HC, Harrison R, Lewis O, Pritchard G, Howell M, Irving C, Johnson D, Kinch S, Marshall C, Lawrence AD, Blinder S, Sossi V, Stoessl AJ, Skinner P, Mohr E, Gill SS.
Journal: Brain, 2019: 142; 512–525
PMID: 30808022 (This report is OPEN ACCESS if you would like to read it)
In this study, the researchers began by screening individuals to identify those appropriate for the study. Between October 2012 and April 2015, 196 inidividuals from throughout the UK were screened. Of these, 41 individuals were selected to take part in the study. The investigators began the study with a small pilot group of participants (6 people) to assess the safety of the surgical technique and the administration of the GDNF. Once optimised, the remaining 35 participants were given the surgical procedure. All of the participants were then randomised and treated for 40 weeks with either GDNF or the placebo treatment (Click here to read more about the details of the trial).
The primary endpoint of this trial was the percentage of change from the baseline measure in the practically-defined OFF state UPDRS motor score (part III) after 40 weeks of double-blind treatment. This means, how the degree of improvement in participants when they are not on their medication, between the start of the study and the end of the study. Clinical assessments were conducted at the baseline, 8 weeks, 16 weeks, 24 weeks, 32 weeks, and 40 weeks timepoints.
The secondary endpoints of the study included:
- The percentage of change between baseline and the Weeks 40 timepoint in UPDRS motor score in the ON state (that is, the motor performance of participants while on medication)
- The percentage of change from baseline in UPDRS activities of daily living scores in the OFF and ON state
- The UPDRS parts I and IV scores
- The change between baseline to the Week 40 timepoint in Parkinson’s diary ratings.
In addition to these, numerous supplemental endpoints were also measured, including Fluorodopa brain imaging. The imaging was conducted at baseline (before treatment) and again at the 40 weeks timepoints.
The results of the study suggest that there was no difference in OFF or ON performance at the 40 week timepoint between the GDNF and placebo treated group. As you can see in the graph below, both group began improving soon after treatment began, and they both continued to do so across the 40 weeks of the study. A decrease in UPDRS score suggests an improvement in the motor performance of the participants, and both the red line (GDNF treatment) and the blue line (Placebo group) on the graph have a downward tragectory.
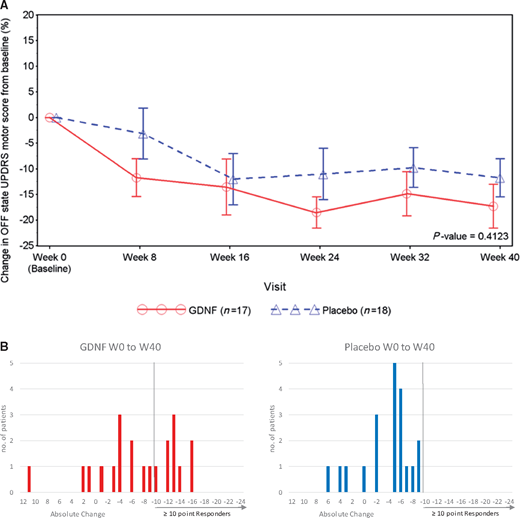 Source: Brain
Source: Brain
Admittedly, the red line is lower than the blue line, but this never gets statistically significant.
How do we explain this?
There may be a difference of opinions here, but I would lean towards a placebo response.
What is a placebo response?
A placebo response occurs when one exhibits a reaction to a treatment, for which there is no pharmacological reason. There is no biological reason why the placebo treatment caused the control group to improve, but they did.
In addition, none of the secondary endpoints exhibit any significant differences between the two groups.
This is really bad right?
It is unfortunate, but it is not the end of the world.
More importantly, there some very interesting findings in the overall results.
Such as?
The responders.
Que?
Every drug trial has individuals who respond better than anyone else in the study, and this study was no different. Some members of the GDNF treated group responded better than others to the treatment.
But crucially, this ‘responder difference’ points towards a difference between the GDNF and placebo group.
You see, when the researchers looked at number of participants who achieved a better than 10 point improvement on the OFF UPDRS score, there were 9 who experienced this in the GDNF group, but none in the placebo treated group. While there were many individuals who had a placebo response in the control/placebo group, none of them had a response as big as the GDNF responders.
And you can see this is the graphs below. On the left (GDNF treated group), there are 9 red bars beyond the >10 point responder line, but on the right (blue) side there are none.
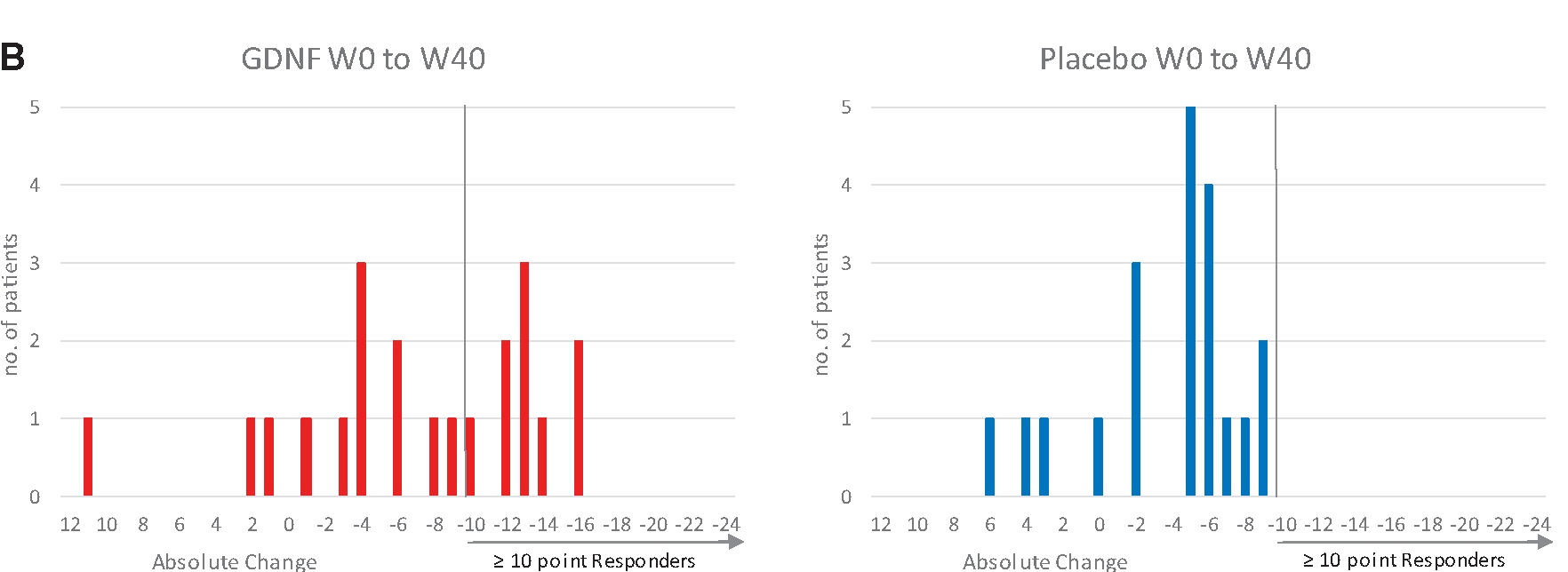 Source: Brain
Source: Brain
Interesting. Anything else of interest?
Yeah: The brain imaging results.
Have a look at the image below:
 Source: Brain
Source: Brain
Each of the 4 green circles represents a birds-eye view of the brain. The red/yellow regions are the putamen on each side of the brain, and the greater the intensity of red colouration, the greater the level of dopamine activity. Now, if you look at the two brains in the top row, these are images from the same individual (baseline image on the left and 40 week image on the right). Note the subtle reduction in red colouration in the right (40 weeks) image compared to the left (baseline) image (particularly around the bottom tips of the putamen). This loss of red colouration suggests a reduction in dopamine activity. The images in the top row came from an individual who was treated with the placebo during the study.
Now shift your attention to the bottom row of brain images, and note the increase in red colouration in the right hand image (the 40 week timepoint). I hope you will agree that compared to the baseline image (left), there is a lot more red colouration on the 40 weeks (right) image. This difference suggests an increase in dopamine activity.
What could the brain imaging results mean?
It suggests that the GDNF was having a biological effect in the brain – the treatment was doing something. Exactly what that ‘something’ is still needs to be determined.
There are in effect three possible explanations:
1. There is an increase in dopamine turnover in the remaining dopamine fibres
2. There is an increase in the number of dopamine fibres
3. There is an increase in other types of neuronal fibres which can take up Levodopa
All three explanations are possible. But we currently have no means of testing which is the answer – beyond repeating the experiment with a larger range of brain imaging assessments.
But I hope you will agree that this is a very interesting part of the results and it certainly deserves further investigation.
Interesting. Anything else?
One other really interesting detail in the results: No antibodies.
Across both the double-blind and open label parts of the study, the researchers never detected any antibodies against GDNF in the analysed blood of participants at anytime during this study.
(NOTE: After the 40 weeks of double blind study, there was another 40 weeks of open label assessment in which all of the participants received GDNF – Click here to read the report on that phase of the study).
So what happens next?
Well, this does not appear to be the end of GDNF or neurotrophic therapy approaches for Parkinson’s.
There are a lot of ongoing discussion regarding whether there should be another trial to follow up the responder data and the brain imaging results. There are questions being asked as to whether the dose of GDNF was high enough to have an effect – the dose used was 3.5-fold smaller than in the historic continuous dosing studies (120 µg versus 420 µg), for safety reasons based on the neurodegenerative results from primates. In addition, some folks are asking if the study was long enough.
And while these discussion regarding GDNF continue, we should get some news soon about another neurotrophic factor clinical study which is using the same delivery system as the Bristol GDNF study. The cerebral dopamine neurotrophic factor (CDNF) clinical trial being conducted in Finland and Sweden is scheduled to finish this year, and we will hopfully get some news about that study. This study is being run by the biotech firm, Herantis.
![]() The Phase I/II study is evaluating the safety and tolerability of CDNF in people with Parkinson’s. Similar to the Phase II GDNF study, the drug is injected directly into the brain using an implanted canular system. One-third of the participants have received monthly infusions of placebo and two-third of the participants have received monthly infusions of either mid- or high-doses of CDNF for 6 months (Click here to read more about this trial). An extension study of this trial has recently been initiated (Click here to read more about that study).
The Phase I/II study is evaluating the safety and tolerability of CDNF in people with Parkinson’s. Similar to the Phase II GDNF study, the drug is injected directly into the brain using an implanted canular system. One-third of the participants have received monthly infusions of placebo and two-third of the participants have received monthly infusions of either mid- or high-doses of CDNF for 6 months (Click here to read more about this trial). An extension study of this trial has recently been initiated (Click here to read more about that study).
The topline results from this study will not be available until next year, but the safety/tolerability data from this trial are going to be presented the Alzheimer’s/Parkinson’s 2019 meeting in March. It will be interesting to see what those results suggest.
In addition to this study, there is a gene therapy GDNF clinical trial starting in California. This study was originally supposed to be conducted on the east coast of the US, but it has been shifted to the west coast, and it will hopefully be starting in the summer. This study will involve an AAV virus being injected into the brain, which will infect cells with the DNA required for the production of GDNF – causing cells in a particular region of the brain to start producing GDNF (Click here to learn more about this trial). We will be keeping an ear to the ground for information relating to this study.
And on top of this, there is also a company called Genecode, which is developing orally delivered “small molecules that mimic GDNF and trigger neurotrophic signalling in dopaminergic neurons” (Source). It will be interesting to see what happens with this company.
 Phew, Long post! So summing up. What does it all mean?
Phew, Long post! So summing up. What does it all mean?
Not just yet.
There is somethings else we really need to discuss.
There is no way of avoiding the fact that there was an enormous placebo response in the control/placebo-treated group in this study. As I mentioned above, a placebo response occurs when one exhibits a reaction to a treatment, for which there is no pharmacological reason. There was no biological reason why the placebo treated group should have improved, but they did.
Some folks might suggest that the surgical procedure instills a strong chance of placebo effect. Others will point towards the excellent and dedicated clinical care at a single research site (which was committed to maximising patient retention) possilby aiding this situation. While I am open to theories or ideas as to what could have caused the placebo response, I am biased towards a more human answer: This trial started with some mighty big expectations on the part of everyone involved (both the participants and the coordinators).
And this potential for a placebo response deeply concerns me as we start to put further resources towards large clinical trials for treatments that the community already has high expectations for (think: Exenatide). Placebo response is acknowledge as a problem in Parkinson’s (Click here to read an old SoPD post about this), and the Bristol GDNF study provides a fine example of it.
We need to have a careful think about managing expectations going forward.
So what does it all mean?
I hope I will be forgiven for using the rollercoaster analogy in this post, but I have watched the GDNF saga from the sidelines since starting my PhD in 2002. The lab I conducted my doctoral research in was one of many that produced some of the early preclinical GDNF data, so I was surrounded by the buzz of excitement about this amazing new compound. I have read the “Monkeys in the middle” book by Nick Nelson (a very good, but slightly dated review of the GDNF story), and I have followed every subsequent twist and turn of this tale.
I like to think that have provided a fair overview of the GDNF story and description of the latest clinical trial results in this post (and I am happy to be corrected on any details).
But please understand, there is a terrible sense of having been to this rodeo before.
Of having watched the rollercoaster do the loop-the-loop several times.
God all mighty, it’s deja vu all over again.
There are going to be lots of voices in the aftermath of these results being published, and my hope is that unlike many previous unsuccessful clinical trials which have been swept under the rug and forgotten (40% of Parkinson’s clinical studies do not publish their results – Click here for more on that rather damning statistic), I hope that the Bristol GDNF clinical trial will be the trigger for change.
An acknowledgement by the entire community that our clinical trial process needs to be carefully reconsidered and adapted. A very sober analysis of the Bristol GDNF study is required. It should involve voices from all sides of the clinical trial process. Patients, clinicians, everyone. A constructive conversation about how we can improve things and do better. Please let us learn from this experience, and use that knowledge to plan for better – and ideally more successful – future clinical trials.

EDITOR’S NOTE – The author of this post is an employee of the Cure Parkinson’s Trust and the President of his local Parkinson’s UK support branch. Both of these organisations – the Cure Parkinson’s Trust and Parkinson’s UK – funded the Bristol Phase II clinical trial of GDNF in Parkinson’s. Neither organisation nor the GDNF team at Bristol Hosptial have asked for this post to be written. This post has been provided by the author solely for the purpose of sharing what he considers to be an interesting story of medical research.
The banner for today’s post was sourced from the Cure Parkinson’s Trust